The Role of Extracorporeal Septorhinoplasty in Severely Deviated Noses: A Prospective CrossSectional Study
ABSTRACT
Introduction: Patients with gross septal deviations often present with both aesthetic and functional problems, demanding precise preoperative evaluation and accurate surgical planning. Managing such gross septal deviations often present technical surgical challenges. Extracorporeal septorhinoplasty (ECS) is a reliable solution for treating severely deviated noses. This study aims to assess the functional and aesthetic outcomes of ECS in patients with markedly deviated noses.
Methods: This prospective cross-sectional study, conducted at Kathmandu Medical College between February 2023 and April 2025, evaluated patients with severe nasal deviation treated using the ECS technique. Nasal obstruction was assessed pre- and postoperatively using a Visual Analog Scale (VAS), while anthropometric parameters such as nasofrontal, nasolabial, and external deviation angles were analyzed from standardized photographs taken six months after septorhinoplasty.
Results: Among 68 patients (43 males, 25 females; aged 18–48 years) who underwent extracorporeal septoplasty, the mean operative time was 115 minutes. Postoperatively, all patients achieved a nearstraight septum with significant improvement in nasal obstruction (VAS 8.41 ± 1.05 pre-op to 1.76 ± 0.99 at 6 months, p < 0.001). Marked aesthetic enhancement was also observed, with statistically significant improvements in the nasofrontal, nasolabial, and external deviation angles.
Conclusions: Extracorporeal Septorhinoplasty offers a definitive solution for gross septal deviations, delivering durable structural correction, improved function, and high patient satisfaction. Continuous refinements and modifications in technique have solidified its role as a reliable approach in reconstructive nasal surgery.
Keywords: Conventional septoplasty, Extracorporeal septoplasty, Polydioxanone plates, Structural stability
INTRODUCTION
Severe nasal deviation is due to birth or childhood trauma, with subsequent asymmetric abnormal
growth leading to the so-called “congenital” twisted nose.[1] Gross septal deviations especially on
dorsal and caudal end of cartilaginous septum which are difficult to treat by classical septoplasty.
Extracorporeal septorhinoplasty (ECS) is an important surgical option for such gross deviations,
enabling complete correction through septal replacement rather than limited reshaping.
Significant trauma in later life can also lead to severely deviated nose, and more rarely it occurs as
a complication following rhinoplasty. Patients complain of both aesthetic and functional problems
as a result of this nasal deformity, which requires careful preoperative evaluation and surgical
planning. In the recent years, new procedures in septoplasty have been presented, however they are
not suitable for massive septal deformities.[2,3,4,5,6]
The objective of this study is to measure the outcomes of extracorporeal septorhinoplasty in severely deviated noses.
METHODS
This prospective cross-sectional study was performed in the department of ENT-HNS at
Kathmandu Medical College from February 2023- April 2025. Approval for ethical clearance was
taken from ethical committee for research and development council of Kathmandu Medical College (Ref. 12082024/16). Written consent was taken from all the patients undergoing extracorporeal septorhinoplasty. All the patients with severely deviated nose having both aesthetic and functional problems who underwent septorhinoplasty using the ECS technique during study period were included in the study.
Patients undergoing revision rhinoplasty, patients having nasal polyposis, patients with Body
Dysmorphic Disorder (BDD) and those patients who were unable to do follow-up were excluded
from the study. Convenience sampling methods was used where all 68 patients with severely deviated noses with age ranging from 18-48 years seeking for septorhinoplasty using the ECS technique were
included in the study.
Data were entered in Microsoft Excel and analyzed using SPSS vs 20. Descriptive statistics were
described by mean, median, standard deviation (SD) and interquartile range (IQR). Inferential
statistics were performed using paired t-tests. A significance level of α = 0.05 was considered for all
statistical analyses.
Surgical technique
All the patients underwent extracorporeal septorhinoplasty (ECS) under general anaesthesia
with an open approach. Preoperatively 3D CT scan (Computed Tomography) with multiple images
from different angles to create detailed, interactive three-dimensional models of nasal framework, for
diagnosis and treatment planning was done. ECS was planned preoperatively when the patient had
severe septal deviation seeking for aesthetic and functional improvement. The osseocartilaginous
skeleton was exposed with an open approach using inverted V incision, and the septal mucoperichondrial flaps were elevated. The entire septal cartilage was removed leaving behind about
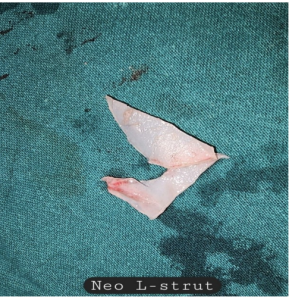
10 mm of the dorsal stump in situ to avoid injury to the keystone. Twisted septal cartilage was then cut
along the maximum deflection angle, and the neo L strut was rebuilt with an optimal tip projection
and pleasant dorsal profile (Figure 1). The posteroinferior portion of the septal cartilage was
used for caudal strut as this portion of cartilage is straighter and stronger. Different types of
osteotomies were done prior to reinsertion of the septal cartilage. The neo-L strut was then
reimplanted and fixed to the dorsal stump and to the soft tissues around the anterior nasal spine (ANS)
in the middle using 5-0 polydioxanone (PDS) sutures.
Additional spreader grafts were shaped in rectangular bars from harvested septal cartilage,
approximately 2–3 cm long, 3–5 mm wide, and 1.5 mm thick and were inserted either unilateral or
bilateral to stabilize the dorsal support and camouflage the defect in all the cases. Dorsal part
of the septal cartilage was reconnected to the upper lateral cartilage with 5-0 PDS. Trans-septal
mattress (quilting) sutures using 4-0 vicryl was placed through the septal mucosa to avoid septal
hematoma. Tip definition was secured by transdomal and interdomal suturing using 5-0 PDS.
Additional tip onlay graft was added if required to improve tip definition. Finally, the skin incision was closed with 6-0 nylon sutures and external nasal splints were applied for 1 week. All the
patients were discharged on the second postoperative days. Swelling and bruises around the
eyes were seen for 3-5 days. Patients also complained of nasal congestion for 4-5 days. Suture
and external splint removal was do after 7-10 days of surgery.
Nasal obstruction symptoms were evaluated preoperatively and postoperatively using a visual
analog scale (VAS) graded from 0 means (no discomfort) to 10 (maximal symptoms).
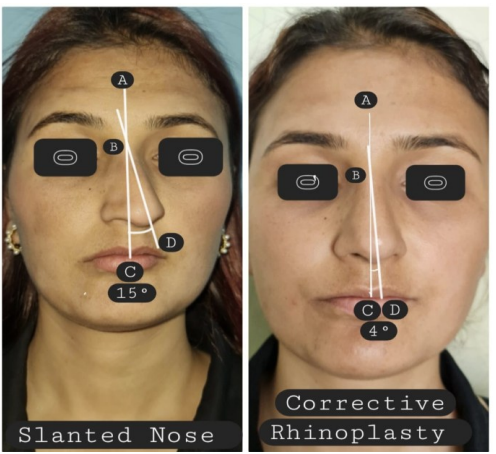
Anthropometric changes such as nasofrontal angle (NFA), nasolabial angle (NLA) and external
deviation angle were assessed preoperatively and postoperatively using facial photographs taken 6
months postoperatively (Figure 2). The preoperative and postoperative degree of nasal
obstruction and anthropometric measurements of the nose were analysed by using paired t-tests
(SPSS ver. 20).

RESULTS
This study included 68 patients (43 males and 25 females) with age ranging from 18-48 years who
underwent rhinoplasty using the ECS technique. The mean operative time from incision to external
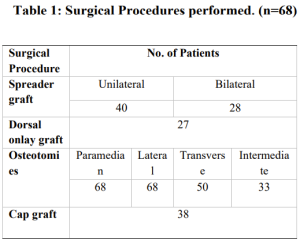
splinting was 115 minutes. The concomitant procedures are listed in (Table 1). The neo-L strut
graft was used for structural support, along with bilateral spreader graft in 28 cases and unilateral in
40 cases. Dorsal onlay septal graft was used in 27 cases. Different types of osteotomies (paramedian,
lateral, transverse, intermediate) was done in all the cases. Cap graft was used in 38 cases for making the
tip more projected and defined.
Nasal endoscopy revealed almost straight septum in all patients postoperatively, and the VAS scores for
nasal obstruction were (8.41±1.05) preoperatively and (2.11±1.09), (1.76±0.99) respectively in 3, 6
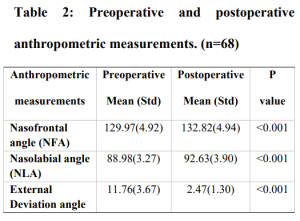
months postoperative period (P<0.001). The mean NFA was 129.97(4.92)0 preoperatively and
132.82(4.94)0 postoperatively (P<0.001). The mean preoperative NLA was 88.98(3.27)0 and
92.63(3.90)0 postoperatively (P<0.001). Significant changes in postoperative values of NFA and NLA
was seen in our study. The postoperative change in the external deviation angle was also statistically
significant 11.76(3.67)0 preoperatively to 2.47(1.30)0 postoperatively, (P<0.001) (Table 2). No major postoperative complications such as infection, saddling and change in shape of nose to its original one were seen in 6 months follow-up period. Small perforation (<1cm) was seen in 3 patients. In addition, there were no revision cases.
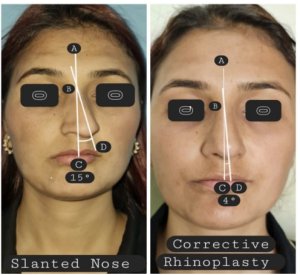
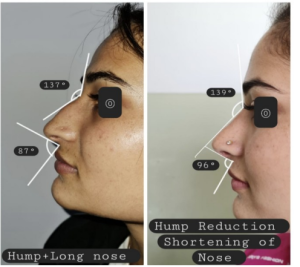
Figure 2: Showing anthropometric measurements of External deviation, Nasofrontal and Nasolabial angles.
DISCUSSION
In septorhinoplasty (SRP), septoplasty serves three crucial purposes such as straightening of dorsal and
caudal septum, reestablishing robust structural support, and providing essential graft material for
sculpting the nasal framework. [7,8] A severely deviated septum retains an inherent elastic
“memory,” making definitive correction a considerable surgical challenge. Conventional septoplasty techniques, such as scoring, often fail to overcome the cartilage’s natural tendency to recoil
to its original form. This phenomenon underscores the inherent limitations of traditional septoplasty in
achieving stable, long-term correction of severe septal deformities. Extracorporeal septorhinoplasty
(ECS) has emerged as a highly effective approach for managing severe nasal deviations, providing
superior functional improvement and comparable aesthetic refinement to that achieved with
traditional septoplasty in rhinoplasty.[9]
To overcome this issue, extracorporeal septorhinoplasty (ECS) was introduced by Gubisch in 1995 as a reliable surgical option for correcting markedly deviated septum. In this technique, instead of weakening bent cartilage, ECS involves complete removal of the septum, straightening it externally, and reimplanting it as a new structural framework.[10] The memory of cartilaginous septum is eliminated and more durable correction is achieved. A large series of Gubisch demonstrated that ECS consistently improves both nasal function and aesthetic outcomes, particularly in patients with complex C- and S-shaped deformities.[11] Lee et al. [12] found that patients who underwent ECS had significantly fewer residual symptoms of nasal obstruction compared to those treated with conventional septoplasty. Although, ECS can be used to accomplish all three pivotal goals of septoplasty, however there is possibility of septal perforation due to submucosal bilateral tunneling in ECS.[13] This is in accordance to our study we found septal perforation in three patients.
Functional outcomes following ECS are well established in the literature. A systematic review of
17 studies involving 1,418 patients reported significant improvements in nasal airflow, 70%
increase in airflow on rhinomanometry, with mean NOSE score reduction from 75 preoperatively to
19.5 postoperatively.[14] In three years follow-up period, Fahmy et al. observed a median reduction in
NOSE score from14.5 to 3.0, confirming the durability of symptom improvement.[15]Dramatic
improvement in both nasal obstruction and cosmesis after anterior septal reconstruction in
patients with severe caudal deviation was documented by Toriumi and Becker.[16] Similarly,
in our study we found significant improvement in nasal obstruction , the VAS score was (8.41±1.05)
preoperatively and (2.11±1.09), (1.76±0.99) respectively in 3, 6 months postoperative period
(P<0.001).
The concept of facial aesthetic triangles given by Powell and Humphreys describes the ideal range for
Nasofrontal angle as 115–130°.[17] Radix augmentation can improve the angry look of the
patient or ameliorate the appearance of a wide intercanthal distance. A low radix can produce a
flattened, wide and washed-out face; appropriate projection of this area by augmenting the profile
and framing the eyes makes a more beautiful appearance.[18] Our study, showed increment of
nasofrontal angle (NFA) from 129.97(4.92)0 preoperatively and 132.82(4.94)0 postoperatively
by augmenting the radix area with crushed septal cartilage graft, thus maintaining the ideal NFA.
Study done by Sinno et al. [19] found that the ideal and most aesthetic nasolabial angle (NLA) ranged
from 100.9 to 108.9 degrees in the female nose and 90.7 to 103.3 degrees in the male nose. Likewise, in our study, the mean average preoperative NLA was 88.98(3.27)0 which increased to 92.63(3.90)0
postoperatively, thus maintaining the ideal NLA. A study done by Jo et al. [20] found that in the frontal
view, external deviation angle differences from preoperatively 5.79 ± 3.36 degrees to postoperatively 1.07 ± 1.24 degrees (P < 0.05).
Similarly, we found statistically significant differences in external deviation angle from 11.76(3.67)0
preoperatively to 2.47(1.30)0 postoperatively. Recent innovations continue to enhance the outcome of ECS. Study done by Nivas et al. compared ECS using absorbable polydioxanone (PDO) plates with conventional septoplasty in 100 patients and reported superior nasal patency, lower complication rates, and higher patient satisfaction in the ECS group.[21] Such adjunct helps in improving fixation stability and further reduce relapse or septal perforation risks. Taken together, these findings establish ECS as the most reliable technique for correcting severely deviated septum.
It addresses the problem of cartilaginous memory, providing more durable structural support, and
consistently yields superior functional and aesthetic outcomes compared with traditional septoplasty.
Though technically demanding, advancement in fixation techniques and use of adjunctive materials
have improved its safety and reproducibility, reinforcing ECS as a foundation in treating gross
septal deformities.
CONCLUSIONS
In conclusion, the ECS technique in septorhinoplasty achieved effective and reliable results in terms of esthetic and functional outcomes thus confirms the validity of this procedure in treating the patient with severe septal deviation rather than conventional septoplasty.
REFERENCES
1. Van Olphen AF. The septum. In: Gleeson M, Browning GG, Burton MJ et al, editors. Scott-Brown’s
otorhinolaryngology, head and neck surgery, 7th edition. London: Hodder Arnold; 2008. p. 1569.
2. Guyuron B, Uzzo CD, Scull H. A practical classification of septonasal deviation and an effective guide to septal surgery. Plast Reconstr Surg. 1999; 104: 2202-2212. [DOI]
3. Thatte RL, Deshpande SN, Thatte MR. A radical approach in the treatment of the deviated nose. Br J Plast Surg. 1990; 43: 596-602. [DOI ]
4. Godfrey NV. Sagittal section septoplasty: an intrinsically stabilized septoplasty. Plast Reconstr Surg. 1994; 93:188-196. [DOI]
5. Mantovani M, Mazzola RF, Cioccarelli MG. The back-and-forth septoplasty. Plast Reconstr Surg. 1996; 97: 40-44. [DOI]
6. Numanoglu A. External cantilever sling in septorhinoplasty: a new technique. Plast Reconstr Surg. 1997; 100: 250- 256. [DOI]
7. Won TB, Kang JG, Jin HR. Management of post-traumatic combined deviated and saddle nose
deformity. Acta Otolaryngol. 2012 Jun;132 Suppl 1: S44-51. [DOI]
8. Jin HR, Kim DW, Jung HJ. Common sites, etiology, and solutions of persistent septal deviation in revision septoplasty. Clin Exp Otorhinolaryngol. 2018 Dec;11(4): 288-92. [DOI]
9. Lee SB, Jang YJ. Treatment outcomes of extracorporeal septoplasty compared with in situ septal correction in rhinoplasty. JAMA Facial Plast Surg. 2014;16(5):328-34. [DOI]
10. Gubisch W. The extracorporeal septoplasty: a technique to correct difficult nasal deformities. Plast
Reconstr Surg. 1995; 95(4): 672-82. [DOI]
11. Gubisch W. Twenty-five years experience with extracorporeal septoplasty. Facial Plast Surg. 2006; 22(4): 230-9. [DOI]
12. Lee SB, Jang YJ. Treatment outcomes of extracorporeal septoplasty compared with in situ septal correction in rhinoplasty. JAMA Facial Plast Surg. 2014 Sep-Oct;16(5):328-34. doi: [ DOI]
13. Kantas I, Balatsouras DG, Papadakis CE, Marangos N, Korres SG, Danielides V. Aesthetic reconstruction of a crooked nose via extracorporeal septoplasty. J Otolaryngol Head Neck Surg. 2008 Apr; 37(2):154-9. [PMID: 19128604]
14. Jang YJ, Kim H, Kim J, Kim HS. Functional outcomes and complications after extracorporeal septoplasty: a systematic review. Laryngoscope. 2020;130(1): E12-20.
15. Fahmy FF, Patel NR, Watson D, Alam MS. Extracorporeal septoplasty outcomes: a retrospective study of 50 patients. Eur Arch Otorhinolaryngol. 2015;272(7):1689-94.
16. Toriumi DM, Becker DG. Anterior septal reconstruction for treatment of severe caudal septal deviation. Laryngoscope. 1999;109(8):1255-62.
17. Powell N, Humphreys B. Proportions of the aesthetic face. Stuttgart: Thieme Publishing Group; 1984. [Google Scholar]
18. Becker DG, Pastorek NJ. The radix graft in cosmetic rhinoplasty. Arch Facial Plast Surg 2001; 3:115-9. [ DOI]
19. Sinno HH, Markarian MK, Ibrahim AMS, Lin SJ. The ideal nasolabial angle in rhinoplasty: a preference analysis of the general population. Plast Reconstr Surg. 2014 Aug;134(2):201-210. [DOI]
20. Jo Ki Hun; Lee, So Yeon; Kwon, Jae Hwan; Kim Jooyeon. Sequential Assessment of External Nasal Deviation Angle Changes in Patients With a Deviated Nose Who Underwent Bilateral Osteotomy. The Journal of Craniofacial Surgery 35(4): p 1231-1235, June 2024. | [DOI]21. Nivas RP, Theivanai S, Shivakumar S, Karthikeyan B. Comparison of Extracorporeal Septoplasty with
Polydioxanone Plates Versus Conventional Techniques for Managing Complex Nasal Septum Deviations. J Pharm Bioallied Sci. 2025 May;17(Suppl 1):S299-S301. [DOI]